Disciplines HCI
Introduction
Currently, VR Exposure Therapy (VRET) for phobias is slowly becoming accepted by therapists in the field. Several studies have shown VRET to be effective in treatment of acrophobia, claustrophobia, fear of flying and other phobias. For therapists to be able to use the VR equipment in an efficient and effective manner, research is needed into the Human-Computer Interaction (HCI) typical for such systems.
Not much previous research exist on the usability of (immersive) VR systems, which makes it an interesting topic.
Research Structure
The first step has been to create a task analysis. This analysis was based on three types of information:
- Observations of therapists using current state-of-the-art VR tools
- Analysis of psychology literature
- Interviews with therapists in the field
A testbed was created capable not only of generating the virtual worlds necessary for treatment, but also enabling the use of different types of user interfaces both for the patient and the therapist. Based on an analysis of currently available systems, a typical User Interface (UI) was developed and used by therapist to treat fear of heights. These therapy sessions were videotaped and analysed. Based on the task model, several key areas for improvement of the HCI have been identified. A number of design alternatives have been created to improve the usability of VRET systems. The research also include field observations of VRET sessions. The aim is to develop a more generic user interface.
Alternatives for the therapist UI
VRET systems typically show the same image to the therapist and the patient. Using our VR testbed, we have created a seperate screen for the therapist.
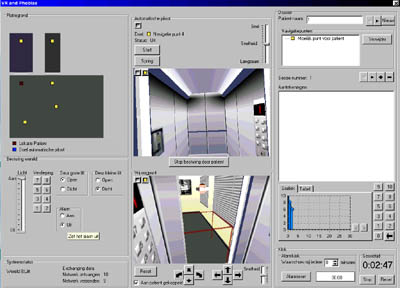
User Interface for the therapist
Based on the task analysis, several elements have been incorporated into this UI to facilitate the work of the therapist. The screen shows the viewpoint of the patient, but also a second viewpoint. This second viewpoint shows the location of the patient in the virtual environment by displaying a virtual Head Mounted Display (HMD) on the location of the viewpoint of the patient. Furthermore, the railing that surrounds the patient in reality is also depicted in this viewpoint. This way the therapist can determine whether the real railing coincides with a virtual railing, creating the illusion that the patient can grab the virtual railing and look over it.
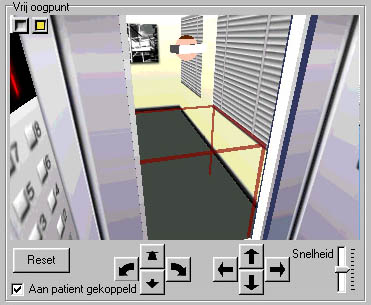
Second viewpoint for the therapist, showing the location of the HMD and the railing surrounding the patient
Furthermore, the screen shows a tool for recording Subjective Units of Discomfort (SUDs),which is a rating for the fear a patient is experiencing. Also, a map of the virtual environment, complete with navigation points and autopilot is available for the therapist. The therapist can control elements of the virtual environment through use of several 2D controls such as buttons and sliders.
Alternatives for the patient UI
An important aspect of the patient's experience is the sense of presence (s)he is experiencing. Presence is defined as the feeling of being present in the virtual world. We are currently investigating the effect of the HCI on the presence the patient experiences, and the relationship between presence, the fear experienced by the patient and the effectiveness of the therapy. In general, it is believed that more interaction leads to higher presence and thus to higher fear and effectiveness of the therapy. One important type of interaction in VRET is navigation. There are several possibilities for navigating through a virtual world. We have evaluated the following:
- No navigation. Here, the therapist navigates the patient
- Gaze directed. The patient can move in the direction (s)he is looking by clicking a button on a hand-held device
- Hand directed. The patient can move in the direction (s)he is pointing the hand-held device
- Range. The patient can move by stepping closer to the railing
- Walk-in-place. The patient can move by making a walking motion